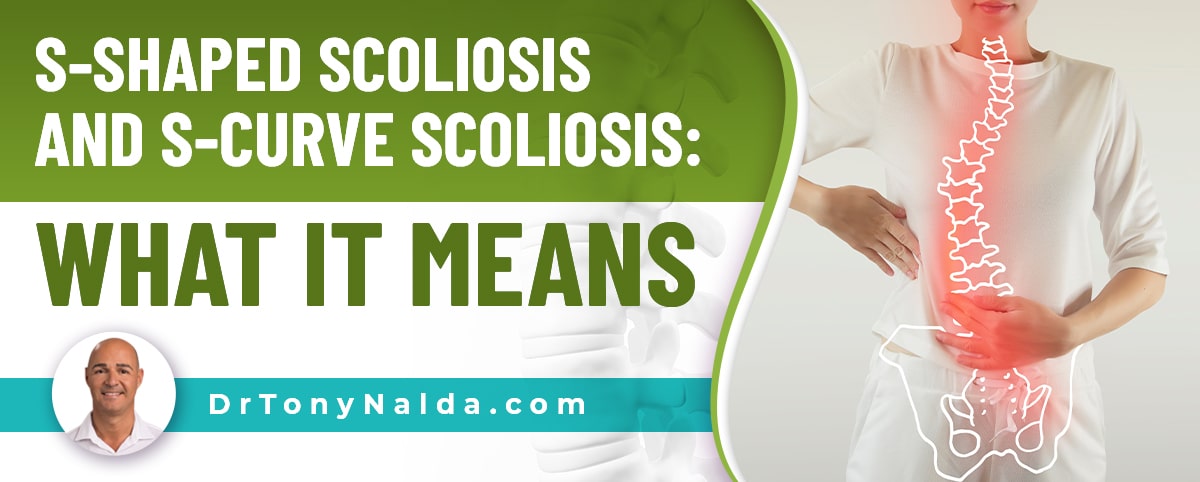
S-Shaped Scoliosis and S-Curve Scoliosis: What It Means
Scoliosis is the development of an unnatural spinal curve that also rotates, and typical cases involve a single c shaped curve, but in atypical condition types, there can be more than one unnatural spinal curve, and this means that treatment is going to be more complex and needs to focus on the larger of the two curves first.
Scoliosis is a complex spinal condition that ranges widely in severity and affects all ages; in addition, there are different types of scoliosis curves. While typical cases of scoliosis involve a right-bending single curve, an s shaped scoliosis, also known as a double curve, bends in opposite directions.
When scoliosis is diagnosed, part of the process involves further classifying conditions based on important patient and condition factors, one of which is curvature location and type, so let's start with how, and why, conditions are classified.
Table of Contents
Classifying Scoliosis
If scoliosis is diagnosed, an unnatural sideways spinal curvature has developed that also rotates, and comprehensive assessment is an important part of the process so conditions can be classified accordingly.
Classifying scoliosis doesn't just streamline the treatment process, it also helps shape the crafting of effective treatment plans, and conditions are classified based on patient age, curvature location, type, and severity.
Part of the reason scoliosis is often deemed complex to treat, which is why a specialist should be recommended, is because no two conditions are the same, so there is no clear-cut treatment plan that will work for a multitude of patients.
Let's touch on some of the classification points that involve the different condition and curvature types.
Different Types of Scoliosis
There are different scoliosis curvature types that indicate a condition's causation.
The most common type of scoliosis to affect both adults and children is idiopathic scoliosis, and the most prevalent form of scoliosis overall is adolescent idiopathic scoliosis, diagnosed between the ages of 10 and 18.
In fact, approximately 80 percent of diagnosed scoliosis cases are classified as idiopathic, meaning we don't fully understand what triggers the condition's initial onset, but we do know what triggers its progression: growth and development.
Progression means the size of the unnatural spinal curve is increasing, as are the uneven forces scoliosis introduces to the body, and their effects.
The remaining percent of known diagnosed cases are associated with known causes and are considered atypical: neuromuscular scoliosis, degenerative scoliosis, and congenital scoliosis.
Atypical cases are more complex to treat; for example, in cases of neuromuscular scoliosis, an underlying neuromuscular condition has caused the scoliosis to develop as a secondary complication.
Muscular dystrophy, cerebral palsy, and spina bifida are a few of the neuromuscular conditions that can lead to scoliosis.
Curvature Direction and Type
Idiopathic scoliosis is considered typical and involves the development of a single c shaped scoliosis because the spine only bends in one direction.
In addition, typical scoliotic curves bend to the right, away from the heart, known as dextroscoliosis, and atypical curves bend to the left, towards the heart: levoscoliosis.
When I see a left-bending curve, this is a red flag that there is an underlying pathology that caused the scoliosis to develop, and when known, it's a condition's underlying cause that has to be addressed to treat the condition effectively.
So not only do typical curves bend to the right, they also involve a single c curve, and atypical cases can involve curves that bend to the left and/or bend in both directions as a double curve.
Characteristics of an S-Shaped Scoliotic Curve
There are three main spinal sections: the cervical spine (neck), thoracic spine (middle/upper back), and the lumbar spine (lower back).
Scoliosis can develop in any of these sections, but the thoracic spine, as the largest spinal section, is the most commonly affected, and there is also what's known as a combined scoliosis that develops in two spinal sections.
For example, thoracolumbar scoliosis is a common diagnosis: a curve develops in the lower thoracic spine and the upper lumbar spine.
When a curve affects two spinal sections, the section with the larger curve has to be the focus of treatment, and each curve needs to be classified separately based on its severity and location within the spine.
 When an s curve develops, this involves a curve that bends in opposite directions: to the left and to the right.
When an s curve develops, this involves a curve that bends in opposite directions: to the left and to the right.
As scoliosis progresses, the unnatural spinal curve will get more rigid, making it less responsive to treatment; as this occurs, a reduced range of motion in the affected area is likely, and this can disrupt a patient's ability to perform certain therapeutic exercises that are part of treatment.
And as it's not just the spine that has to maintain its natural curves and alignment, but also the spine's surrounding muscles, muscles that are pulled in different directions by the unnatural spinal curve(s), can become unbalanced.
Further Classifying an S-Shaped Scoliosis
In addition to the severity of each curve being determined, location is important because it tells me where to concentrate my treatment efforts, and can also help me predict likely progressive rates and the area of the body that's likely to be the most affected.
Curvature location is assessed by what's known as the plumb line, and as an s-shaped spine presents with two unnatural spinal curves, each curve bends in opposite directions: one to the left, and the other to the right.
 Each curve is classified as a major or minor curve, and the major curve is the larger of the two; in a double curve, one curve will always be more prominent.
Each curve is classified as a major or minor curve, and the major curve is the larger of the two; in a double curve, one curve will always be more prominent.
A lumbar curve tends to be larger than the curves of the thoracic spine, but a thoracolumbar curve can involve the thoracic curve as the more dominant major curve.
Treatment Options for a Double Curve
As a progressive condition, scoliosis is virtually guaranteed to get worse at some point, and while we can't always determine when that will be, we can proactively work towards preventing progression by starting treatment as close to the time of diagnosis as possible.
Remember, with progression comes increasing spinal rigidity, which limits potential treatment efficacy.
Here at the Scoliosis Reduction Center, I apply a conservative chiropractic-centered treatment approach that combines multiple treatment disciplines that can complement one another and counteract the condition's progressive nature.
Treating an s-curve scoliosis is atypical and needs to be comprehensively assessed to determine which curve is the more dominant, and as there are two curves that bend in opposite directions, this generally increases the rotational component.
So once the dominant curve is determined, the first step of treatment has begun, and now, I can start focusing on how to reduce the dominant curve first, and then the lesser curve simultaneously.
As a structural scoliosis, the condition has to be impacted, first and foremost, on a structural level, and I work towards this through condition-specific chiropractic care that involves a series of techniques and manual adjustments that have the goal of realigning the spine.
Once I start to see structural results, I can shift the focus to increasing core strength through condition-specific physical therapy so the spine is optimally supported by its surrounding muscles, posture is improved, and certain areas of the brain are activated for improved brain-body communication.
Corrective bracing can be particularly effective on growing spines, so is a common facet of treatment for scoliosis in children; corrective bracing can help achieve corrective results by pushing the spine into a corrective position, while also addressing the condition's rotational component.
Rehabilitation is the final and ongoing stage of treatment; as a progressive incurable condition, work has to be done to sustain treatment results for the long term, and this involves leading a scoliosis-friendly lifestyle and a series of custom-prescribed exercises for patients to perform at home to further stabilize and heal the spine.
Conclusion
What being diagnosed with an s curve scoliosis, also known as a double curve, means is that a large unnatural spinal curve that rotates and bends in opposite directions, in an 'S' shape, has developed.
This is an atypical type of scoliosis as the scoliotic curve bends in two directions, tends to have more severe rotation, and features a curve that bends to the left, towards the heart.
When I see an s curve, I know that treating two scoliotic curves is going to be more complex, and being proactive with treatment is even more important because the more severe a scoliosis is, the more it's going to progress, and the more likely it is that invasive scoliosis surgery will be recommended in the future.
While spinal fusion has a place in scoliosis treatment, it's neither the best, nor the only treatment option available, and the method isn't aligned with the spine's natural movement-based design, which is why the Center's non-surgical treatment results show that many cases of scoliosis don't require surgery.
Being proactive with treatment means starting it as close to the time of diagnosis as possible, when the condition is going to be its mildest, the spine is going to be at its most flexible, and before the body has had ample time to adjust to the presence of the double scoliosis.
Once the dominant curve is determined, treatment starts there, and then includes the minor curve as both curves need to be reduced on a structural level so as much of the spine's healthy curves as possible are restored.


Dr. Tony Nalda
DOCTOR OF CHIROPRACTIC
After receiving an undergraduate degree in psychology and his Doctorate of Chiropractic from Life University, Dr. Nalda settled in Celebration, Florida and proceeded to build one of Central Florida’s most successful chiropractic clinics.
His experience with patients suffering from scoliosis, and the confusion and frustration they faced, led him to seek a specialty in scoliosis care. In 2006 he completed his Intensive Care Certification from CLEAR Institute, a leading scoliosis educational and certification center.
About Dr. Tony Nalda




 Ready to explore scoliosis treatment? Contact Us Now
Ready to explore scoliosis treatment? Contact Us Now