Scoliosis Degrees of Curvature Chart [ADOLESCENTS & ADULTS]
As a progressive condition, monitoring for increasing condition severity is important, but so is being proactive with treatment so progression can be prevented. The traditional approach believes in a reactive response that commonly funnels patients towards surgery, while a functional approach values being proactive so surgery can be avoided.
Take a look at the accompanying scoliosis degrees of curvature chart for both adolescents and adults, to see how each of the two main scoliosis treatment approaches responds at each severity level; traditional and functional treatment offer patients highly-different potential outcomes.
Adolescents and adults experience scoliosis differently, especially in terms of pain, and the treatment focus can reflect those differences. As adolescent idiopathic scoliosis is the condition’s most-prevalent type, let’s start there.
Table of Contents
Adolescent Idiopathic Scoliosis
Adolescent idiopathic scoliosis (AIS) is diagnosed between the ages of 10 and 18 and is the condition’s most common form.
The idiopathic designation means not clearly associated with a single causative source and is, instead, considered to be multifactorial, meaning caused by multiple factors that can vary from person to person.
One of the important condition characteristics of adolescent idiopathic scoliosis is progression; remember, as a progressive condition, scoliosis has it in its very nature to worsen over time, particularly if left untreated or not treated proactively.
While we don’t fully understand the etiology of AIS, we do understand what triggers the condition to progress: growth and development.
Considering the stage of puberty adolescents are in, or are entering into, this age group is at risk for rapid-phase progression, so monitoring is important, as is being proactive with treatment to try and counteract the condition’s progressive nature.
Where a patient’s scoliosis is at the time of diagnosis is not indicative of where it will stay. A patient diagnosed with mild scoliosis can easily progress to moderate, severe, or very severe, but this can be controlled by the type of treatment, and how the spine responds.
The most important decision a patient, and their families, have to make following an AIS diagnosis is which treatment approach to commit to, so let’s turn to the accompanying adolescent scoliosis degrees of curvature chart to see the difference in how a traditional treatment approach would respond, versus a modern functional treatment approach.
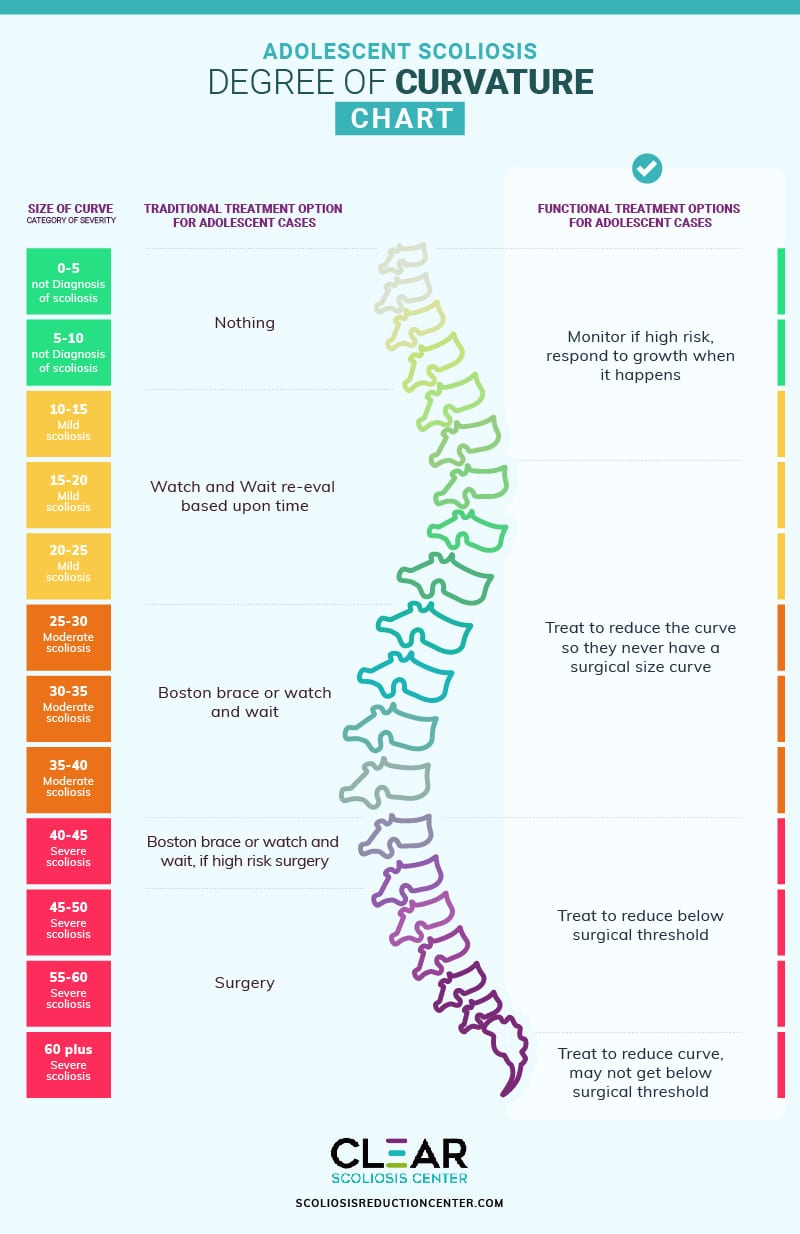
Adolescent Scoliosis Degree of Curvature Chart
Regardless of the treatment approach, the parameters that have to be met to reach a scoliosis diagnosis are the same: an unnatural sideways spinal curve, with rotation, and a minimum Cobb angle measurement of 10 degrees.
Cobb angle is an important measurement obtained during X-ray that determines how severe a condition is:
- Mild scoliosis: Cobb angle measurement of between 10 and 25 degrees
- Moderate scoliosis: Cobb angle measurement of between 25 and 40 degrees
- Severe scoliosis: Cobb angle measurement of 40+ degrees
- Very-severe scoliosis: Cobb angle measurement of 80+ degrees
So now that we know the different severity levels, let’s take a look at the accompanying chart to see how each treatment approach responds at each stage of progression, starting with mild.
Mild Adolescent Idiopathic Scoliosis
Mild scoliosis is diagnosed with a Cobb angle measurement of between 10 and 25 degrees, and this is where the ideologies that govern each treatment approach differ: in how they respond.
There are numerous treatment benefits related to early detection. Although there are never guarantees, but those benefits are only available to those whose treatment providers respond with proactive treatment.
Traditional Treatment
Under traditional treatment, an adolescent patient diagnosed with mild scoliosis is most likely going to be told to watch and wait for further progression to see how/if it progresses.
The issue here is that as a progressive condition, we know virtually every case of scoliosis is going to progress at some point, so merely observing a mild condition can mean allowing a scoliotic curve to progress beyond the mild level.
 Patients are commonly told to return for periodic assessments every 3, 6, or even 12 months (interval-length will depend on the treatment provider), but the risk is that in between these periodic intervals, an adolescent can have a large growth spurt and progress significantly.
Patients are commonly told to return for periodic assessments every 3, 6, or even 12 months (interval-length will depend on the treatment provider), but the risk is that in between these periodic intervals, an adolescent can have a large growth spurt and progress significantly.
Functional Treatment
Under functional treatment, the response to a diagnosis of mild scoliosis is more proactive by starting treatment as close to the time of diagnosis as possible.
I believe that when a condition is mild is precisely the best time to react because when caught early and paired with proactive treatment, there are fewer limits to what we can achieve treatment-wise.
I would craft a customized treatment plan based on important patient/condition variables such as patient age, condition type, curvature location, and severity.
I don’t want to merely observe because I see this as wasting valuable treatment time, and my integrative approach works towards reducing curves so progression is prevented.
Here at the Scoliosis Reduction Center, even while mild, we are already working towards impacting the condition on a structural level while monitoring the spine to see how it’s responding to treatment; that way I can apportion different treatment disciplines accordingly.
Moderate Adolescent Idiopathic Scoliosis
With moderate adolescent idiopathic scoliosis, we’re talking about a Cobb angle measurement of between 25 and 40 degrees, and this is when symptoms like postural changes tend to become noticeable, which is why the majority of patients are diagnosed with moderate scoliosis.
Traditional Treatment
Traditional treatment for moderate scoliosis would continue to involve watching and waiting.
In fact, the only form of treatment applied for moderate scoliosis patients would be traditional bracing; the most commonly-used traditional scoliosis brace in the United States is the Boston brace, which is associated with a number of shortfalls.
The Boston's goal is not correction, but stopping progression, and it does this by unnaturally squeezing the spine into a straighter position, but this can actually weaken the spine over time and increase related postural deviation.
In addition, the Boston doesn’t address the condition’s rotational component, so instead is treating it only in 2 dimensions (side to side), rather than its true 3-dimensional nature (rotational component of front to back, back to front), and this limits its potential efficacy.
Functional Treatment
At 25-40 degrees, we continue to work towards a curvature reduction through a variety of chiropractic techniques and manual adjustments.
Increasing core strength is also important so the spine is optimally supported and stabilized by its surrounding muscles, and this is done through a variety of therapies and scoliosis-specific exercises (SSEs).
We continue monitoring to see how the spine is responding and if the treatment applied is enough to counteract a condition’s progressive rate; the goal is to try and stay ahead of a condition’s progressive line and prevent the need for invasive treatment in the future.
When it comes to adolescents, we want to either reduce their scoliosis, or hold it where it is, throughout the stage of puberty when they are at the highest risk for rapid progression due to growth and development.
Severe Adolescent Idiopathic Scoliosis
At a Cobb angle measurement of 40+ degrees, we are in the severe classification, and at this stage, postural deviation can be overt, and the potential for causing related complications such as digestive issues, sleep troubles, and severe headaches increases.
Traditional Treatment
With traditional treatment, severe adolescent idiopathic scoliosis would be responded to with continued watching and waiting and/or using the Boston brace in an attempt to stop further progression.
This is also the time where patients are often funneled towards spinal fusion surgery as the surgical-level threshold is crossed at 45+ degrees.
If a patient shows signs of continued progression, despite bracing efforts, spinal fusion is commonly recommended as the best remaining treatment option.
Just as all surgical procedures come with their share of risks, spinal fusion is no exception; it’s a costly and invasive procedure that comes with some serious risks and potential side effects, so the procedure warrants a lot of careful consideration.
In addition, while spinal fusion can indeed achieve a straighter spine, the way it’s achieved, through the fusing of bones and rods and screws holding the spine in place, does little for the spine’s overall health, strength, and function.
Functional Treatment
At the 40+ range, functional treatment continues to work intensely towards corrective results in the form of a curvature reduction that would reduce a curve below the surgical-level threshold to avoid surgery.
By combining chiropractic adjustments, rehabilitation, at-home exercises, and corrective bracing, proactive efforts continue to work towards preventing progression and increasing condition severity.
The functional treatment uses a different type of scoliosis brace: the modern corrective ScoliBrace that represents the culmination of what we’ve learned about the condition, and how it responds to treatment, over the years.
The ScoliBrace doesn't just work towards controlling progression, but also has corrective potential as it’s 100-percent customized to suit the patient’s body and condition type, addressing potential compliance issues.
The ScoliBrace also works by pushing the spine into a corrective position, rather than squeezing it unnaturally as does the traditional Boston brace.
At the severe stage, our main goal is to correct the abnormal spinal curve as much as possible, to avoid spinal fusion surgery and its many risks and potential side effects, while preserving as much of the spine’s natural function as possible.
Now, let’s take a look at how the different treatment approaches respond at each severity level with adult scoliosis.
Adult Scoliosis
Although scoliosis is far more commonly diagnosed in children and adolescents, it does also affect adults; the two most common types to affect adults are idiopathic and degenerative.
Cases of idiopathic scoliosis in adults are extensions of adolescents who didn’t receive a diagnosis and treatment in adolescence, and the reality is had these patients received treatment in adolescence, their spines would be in far better shape than by the time they come to see me: highlighting the importance of early detection.
Degenerative scoliosis is caused by natural age-related spinal degeneration, most commonly involving the spine’s intervertebral discs.
An important characteristic of adult scoliosis to understand is progression. Although adults can still progress, once the big trigger of growth has been removed, progressive rates tend to slow, which is why monitoring for rapid progression is not such a focus in adult scoliosis treatment.
Once skeletal maturity has been reached, meaning growth has stopped, scoliosis becomes a compressive condition, and this is why scoliosis is not commonly painful for children and adolescents, but in adults, pain is the number-one symptom, which is why pain management is a focus in the treatment of adult scoliosis, more so than in AIS.
In a young patient who’s still growing, the constant upward lengthening motion of a growing spine counteracts the compressive force of a curvature, and it’s compression of the spine and its surrounding muscles and nerves are the main cause of condition-related pain.
So you can see how different characteristics of the condition can shift the treatment focus in adults versus younger patients.
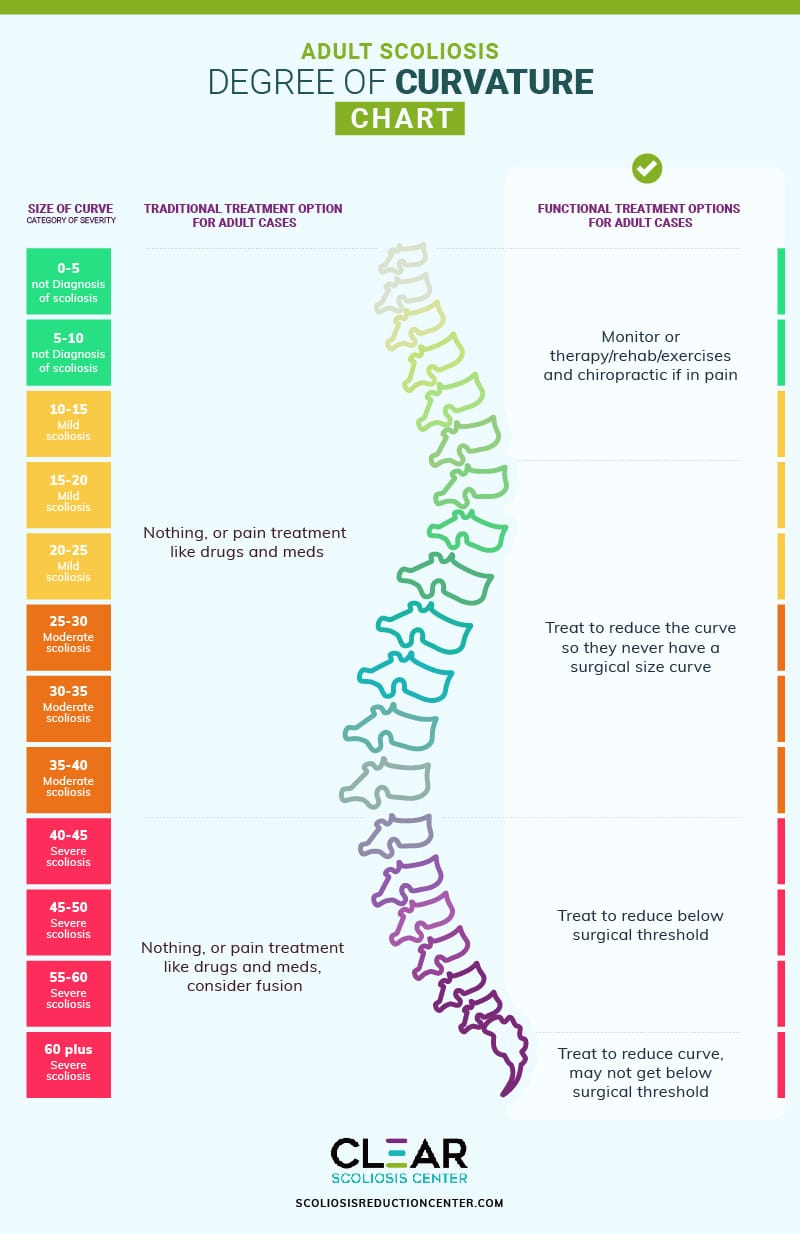
Adult Scoliosis Degree of Curvature Chart
As you can see from the accompanying adult scoliosis degree of curvature chart, the severity levels and corresponding Cobb angle measurements are the same as in AIS, but what you’ll notice is that there is more of a focus on medication as part of treatment: pain management.
While adults aren’t at risk for rapid-phase progression as children and adolescents are, they can still progress, and even at incremental rates of progression, over time, it can add up.
In addition, particularly in cases of degenerative scoliosis, natural age-related spinal degeneration can also come into play, making the spine more vulnerable, and this can increase progressive rates.
In fact, studies show that the rate of scoliosis in adults is between 12 and 20 percent, and in adults 60+ years of age, it’s estimated that scoliosis will be detected in 68 percent of adults.
So while scoliosis is generally regarded more as a child/adolescent condition, the rate of scoliosis actually increases with age.
Let’s now take a look at the accompanying chart to see how the traditional and functional treatment approaches respond at each severity level.
Mild Adult Scoliosis
For adults with a Cobb angle of between 10 and 25 degrees, this is diagnosed as mild scoliosis.
Depending on the chosen treatment approach, this is either when treatment starts, or where it gets delayed.
Traditional Treatment
Under a traditional approach to scoliosis treatment, treatment isn’t started while a condition is mild.
While medications for pain management can be prescribed during this stage, this is doing nothing to treat the actual condition; it’s only addressing pain as a symptom of the condition, but not its underlying cause.
Functional Treatment
For mild scoliosis in adults, I would also be monitoring for progression, but the difference is I would not only be monitoring for progression, but also how the spine is responding to treatment.
A functional approach values proactive treatment, which means starting it as close to the time of diagnosis as possible.
A combination of scoliosis-specific therapy, exercise, and gentle chiropractic care would be used to address the underlying cause of pain in a more effective and sustainable way.
It’s during the mild stage that we would introduce corrective bracing as this can help provide adults with stabilization and support, which also helps with pain and discomfort.
The goal of functional treatment during this stage is to address the underlying structural nature of the condition by working towards a curvature reduction, which would also reduce related symptoms.
Moderate Adult Scoliosis
With Cobb angle measurements of between 25 and 40 degrees, we’re talking about moderate scoliosis.
As in adolescents, the postural changes that scoliosis can cause tend to become more noticeable in the moderate stage, which is why many patients receive their diagnosis after progressing from mild to moderate.
Traditional Treatment
Even at the moderate level, a traditional response would continue to be watching and waiting, combined with pain medications/injections, but again, pain medications do nothing in terms of addressing the underlying cause and only provide short-term relief.
It’s also worth keeping in mind that masking the pain with medications can actually be harmful when it comes to progressive conditions like scoliosis.
While no one wants to experience pain, it does serve a purpose in terms of indicating something is wrong in the body that needs attention.
 If pain medications are masking escalating symptoms, it can be disguising the fact that an adult’s scoliosis is progressing, making treatment more complex and putting them at risk for needing more invasive forms of future treatment.
If pain medications are masking escalating symptoms, it can be disguising the fact that an adult’s scoliosis is progressing, making treatment more complex and putting them at risk for needing more invasive forms of future treatment.
Functional Treatment
Functional treatment for adults with moderate scoliosis would include actively working towards a curvature reduction to restore as much of the spine’s natural curves as possible.
During this time, we are observing the spine, how it’s responding to treatment, and adjusting how we apportion our treatment disciplines: chiropractic care, therapy, rehabilitation, and corrective bracing.
By applying proactive treatment, we are not only addressing symptoms of the condition, such as pain, but we are also impacting the underlying cause of related symptoms by impacting the condition on a structural level.
Severe Adult Scoliosis
For severe scoliosis in adults, we’re talking about curvatures with a Cobb angle measurement of 40+ degrees.
It’s in the severe stage that patients are at risk for developing complications such as digestive issues and lung impairment; while not common parts of the scoliosis experience, if left to become severe and continue progressing, complications are more likely to develop.
Traditional Treatment
Even when severe, the traditional response is to continue pain medication to address symptoms.
In terms of invasive treatment, this is a risky stage to reach because those undergoing traditional treatment are approaching crossing the surgical-level threshold, which means becoming a candidate for spinal fusion surgery.
Again, like all surgical procedures, spinal fusion is risky, but those risks, potential side effects, and complications only increase with age.
Functional Treatment
At 40+ degrees, the goal of functional treatment is to stabilize the spine and reduce the scoliotic curve to below the surgical level threshold, or back to where it was prior to when it started causing noticeable symptoms like pain.
Once that is achieved, we work towards sustaining that reduction to keep symptoms, such as pain, under control while avoiding the need for, and risks of, scoliosis surgery.
Conclusion
I hope you’ve enjoyed following along on the accompanying scoliosis degrees of curvature chart for a visual on how adolescent and adult scoliosis progresses and how the two main scoliosis treatment approaches would respond at each level of progression.
The important thing to remember is that as a progressive condition, merely observing can be quite dangerous; allowing a scoliotic curve to progress unimpeded means allowing it to become more complex to treat, increasing spinal rigidity, making it less responsive to treatment, and allowing the body time to adjust to its presence.
Particularly when it comes to adolescent idiopathic scoliosis, having young patients return at periodic intervals for reassessment is risky because if a significant growth spurt happens in between appointments, this can cause equally-significant progression.
While there are no treatment guarantees, early detection, when coupled with proactive treatment, increases the chance of treatment success, which means avoiding crossing that surgical-level threshold and being funneled towards invasive surgery.
While there is still a place for surgery in scoliosis treatment, the reality is that many cases can be successfully treated nonsurgically.
While a traditional scoliosis treatment approach values a reactive response, a modern functional treatment approach values being proactive with treatment so increasing condition severity, escalating symptoms, and the need for invasive surgery can be avoided.
In addition, a functional approach is designed around the priority of maintaining as much natural spinal function as possible, while spinal fusion is known to cost the spine in terms of its natural flexibility and range of motion.
Here at the Center, I offer patients a functional treatment approach and access to multiple forms of treatment under one roof, where our results speak for themselves.


Dr. Tony Nalda
DOCTOR OF CHIROPRACTIC
After receiving an undergraduate degree in psychology and his Doctorate of Chiropractic from Life University, Dr. Nalda settled in Celebration, Florida and proceeded to build one of Central Florida’s most successful chiropractic clinics.
His experience with patients suffering from scoliosis, and the confusion and frustration they faced, led him to seek a specialty in scoliosis care. In 2006 he completed his Intensive Care Certification from CLEAR Institute, a leading scoliosis educational and certification center.
About Dr. Tony Nalda




 Ready to explore scoliosis treatment? Contact Us Now
Ready to explore scoliosis treatment? Contact Us Now